Mitral regurgitation (MR) is the most common valvular heart disease, and it involves a spectrum of leaflet abnormalities. The Law of Laplace, which describes the tension on muscle fibres in the heart wall, is a critical concept in understanding the mechanisms of MR. According to Laplace's Law, wall stress is proportional to pressure and chamber size and inversely proportional to wall thickness. This law helps explain the relationship between ventricular output and preload, influencing the progression of MR and its treatment options.
| Characteristics | Values |
|---|---|
| Law | Laplace's Law |
| Application | Explains the tension on muscle fibres in the heart wall |
| Calculation | Pressure within the ventricle x Volume within the ventricle / Wall thickness |
| Heart Condition | Mitral regurgitation (MR) |
| Heart Abnormality | Hypertrophic cardiomyopathy |
| Observation | Ventricular output increases as preload (end-diastolic volume) increases |
| Surgery | Corrective surgery is indicated for severe cases |
| Echocardiography | Used to analyse mitral geometry and leaflet motion |
Explore related products






What You'll Learn
![]()
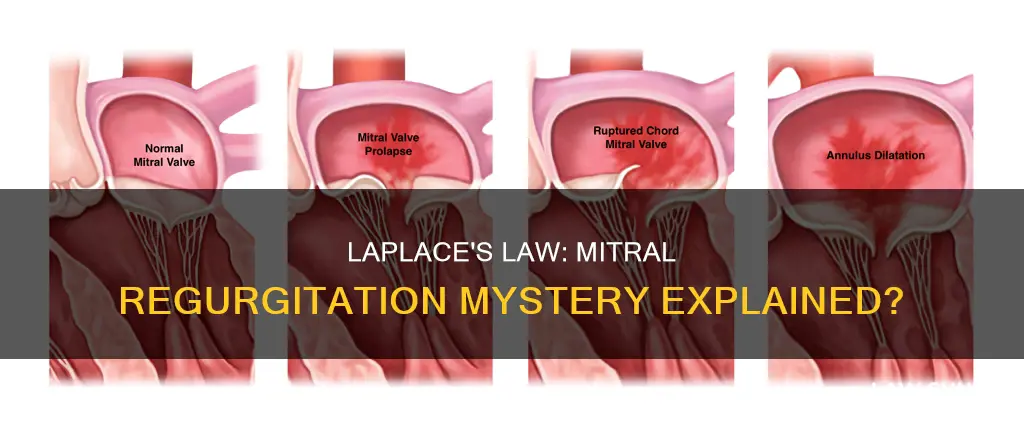
Mitral regurgitation and hypertrophic cardiomyopathy
Mitral regurgitation (MR) is the most common valvular heart disease, and it involves multiple entities. It is caused by the abnormal structure and function of the mitral valve, which can lead to blood flowing back into the left atrium during systole. The severity of MR can be assessed by measuring the volume of the left atrium and the pressure in the pulmonary artery. Echocardiography techniques, such as Doppler measurements, are now primarily used for diagnosis, replacing invasive and angiographic methods.
Hypertrophic cardiomyopathy (HCM) is a type of heart disease characterised by abnormal thickening of the heart muscle, particularly the left ventricle. It is the most frequent monogenic cardiac disease, affecting about 1 in 500 individuals. HCM is associated with systolic anterior motion (SAM) of the mitral valve, which can result in mitral regurgitation. The mitral valve abnormalities in HCM include leaflet elongation, thick leaflets, displacement of the papillary muscle, and systolic anterior motion of the MV anterior leaflet.
In about 70% of patients with HCM, left ventricular outflow tract (LVOT) obstruction occurs due to septal hypertrophy and a pressure drop above the aortic valve. This leads to drag forces that attract the anterior mitral leaflet, frequently causing significant MR. This type of MR is called "SAM-dependent" and is the most frequent form associated with HCM. However, in 10-20% of patients, "SAM-independent MR" can occur due to intrinsic mitral valve abnormalities. In rare cases, MR can be caused by mitral valve chordal rupture associated with HCM, which can significantly impact the patient's prognosis.
Anteriorly directed MR in patients with HCM is considered a red flag for concomitant pathology. While SAM typically results in a posteriorly directed MR jet, an anteriorly directed jet suggests additional mitral valve pathology unrelated to SAM. This type of MR may not be resolved by myectomy alone, and further surgical intervention may be required. Pre-operative echocardiography is essential to detect different MV abnormalities in patients with HCM to guide appropriate treatment.
Lease Agreements: Can They Override State Law?
You may want to see also
Explore related products






![]()
Echocardiography and mitral leaflet motion
Echocardiography has been used to study the mitral valve since the technique's early development. It is a valuable tool in the diagnosis of valvular heart disease, particularly mitral stenosis.
Echocardiography can be used to assess the morphology of the mitral valve leaflets and subvalvular apparatus. In the case of rheumatic mitral stenosis, echocardiography can identify the diastolic doming or hockey-stick shape of the anterior mitral leaflet, which is caused by reduced mobility of the valve tips. The posterior mitral leaflet motion is usually restricted. In the parasternal short-axis view of the mitral valve, leaflet thickening and fusion of commissures and chordae can be observed.
Three-dimensional echocardiography enhances the objective assessment of mitral valve morphology by enabling visualisation of the mitral valve's narrowest orifice through better alignment of the image plane at the mitral tips. It allows for a detailed characterisation of the degree of mitral valve involvement, including leaflet motion, calcification, and commissural fusion, as well as the state of the subvalvular apparatus.
Echocardiography, in combination with Doppler measurements, has largely replaced invasive and angiographic methods in the diagnosis of mitral regurgitation. Two-dimensional and Doppler echocardiography can accurately diagnose the mechanism of mitral regurgitation in patients with posterior leaflet prolapse or flail, anterior leaflet prolapse or flail, bileaflet prolapse or flail, papillary muscle elongation or rupture, restricted leaflet motion or rheumatic thickening, ventricular-annular dilation, and leaflet perforation or cleft.
Overall, echocardiography is a valuable tool in the assessment of mitral valve disease, providing detailed morphological information and aiding in the diagnosis of mitral regurgitation.
California's Resistance: Lawful or Lawless?
You may want to see also
Explore related products






![]()
Mitral regurgitation and ventricular dilation
Mitral regurgitation (MR) is a valvular abnormality that affects over 2% of the population, making it the most common valvular heart disease worldwide. It is caused by the incompetence of the mitral valve, which results in the retrograde flow of blood from the left ventricle into the left atrium during ventricular systole. This leads to an increase in preload delivered to the left ventricle during diastole, causing left ventricular volume overload. As the disease progresses, ventricular remodelling occurs, leading to an enlarged left ventricle chamber.
According to Laplace's Law, wall stress is directly proportional to the pressure and chamber size and inversely proportional to wall thickness. Therefore, in the context of mitral regurgitation, the increased volume overload on the left ventricle results in higher wall stress. This increased wall stress can lead to subendocardial ischemia and subsequent myocardial fibrosis. The left ventricle must generate greater tension to overcome the aortic pressure and eject blood, resulting in a higher afterload.
Ventricular dilation is a significant consequence of mitral regurgitation. The volume overload and increased wall stress contribute to the dilation of the left ventricle. This dilation can lead to further worsening of mitral regurgitation through a positive feedback loop. The dilated ventricle results in a wider mitral annulus, which impairs the coaptation of leaflets, causing more regurgitation over time.
Primary mitral regurgitation, caused by processes such as prolapse, flail, or valve degeneration, can lead to severe volume overload and left ventricular dysfunction. On the other hand, secondary mitral regurgitation is often associated with ventricular dilation, which can be caused by ischemic or non-ischemic cardiomyopathies. The dilation results in apical and lateral papillary muscle displacement, leading to poor coaptation of the mitral leaflets and significant mitral regurgitation.
In summary, mitral regurgitation and ventricular dilation are closely interconnected. Mitral regurgitation leads to volume overload, which causes ventricular dilation, and the dilated ventricle further worsens mitral regurgitation. This cycle contributes to the progression of the disease and the development of left ventricular dysfunction. Understanding the relationship between mitral regurgitation and ventricular dilation is crucial for determining the optimal timing of corrective surgery and preventing irreversible ventricular damage.
Exemptions for Corporations: California Law Execution
You may want to see also
Explore related products






![]()
The Law of Laplace and myocardial oxygen demand
The Law of Laplace states that ventricular wall tension is directly proportional to the ventricular radius and intraventricular pressure. This law helps to understand the mechanics of ventricular wall stress, which is a major determinant of myocardial oxygen demand.
Myocardial oxygen demand refers to the amount of oxygen the heart requires to function optimally. The three factors that determine this demand are heart rate, contractility, and ventricular-wall tension. An increase in any of these variables requires the body to adapt to sustain an adequate oxygen supply to the heart. For example, an increase in heart rate means the myocardium must work harder to complete the cardiac cycle more efficiently, resulting in a higher oxygen demand. Similarly, an increase in ventricular-wall tension, as described by the Law of Laplace, will also increase myocardial oxygen demand.
The Law of Laplace is particularly relevant in understanding the progression of mitral regurgitation (MR), a common valvular heart disease. MR causes eccentric hypertrophy of the left ventricle, leading to systolic and diastolic dysfunction. This results in increased left ventricular end-diastolic volume and pressure, which, according to the Law of Laplace, leads to increased ventricular wall stress. The subsequent increase in myocardial oxygen demand can cause subendocardial ischemia and, if untreated, myocardial fibrosis.
The clinical significance of a rise in myocardial oxygen demand occurs when it exceeds the myocardial oxygen supply. This imbalance can be seen in the later stages of coronary artery disease (CAD). In CAD, the oxygen-carrying capacity of the blood and flow through the coronary arteries, which regulate myocardial oxygen supply, are compromised. Consequently, patients with CAD are advised to avoid situations that lead to large increases in afterload, such as heavy lifting, as it increases arterial pressure and, subsequently, myocardial oxygen demand.
Common-Law Partners: Death Benefits and Your Rights
You may want to see also
Explore related products




![]()
Mitral regurgitation and the Frank-Starling relationship
Mitral regurgitation (MR) is the most common valvular heart disease. It is a complex multifactorial disease that involves multiple entities. The advancement of echocardiographic techniques, such as Doppler measurements, has offered additional diagnostic possibilities and replaced invasive and angiographic methods in daily clinical practice.
The Frank-Starling law of the heart states that the force of ventricular contraction is determined by the degree of stretch on the myocardial fibres just before they contract. In other words, the heart pumps out whatever volume of blood it receives. The preload, or end-diastolic volume, is a prime determinant of the force of contraction because it determines the number of contractile units cycling and the amount of calcium available to permit the cycling. The Frank-Starling law also indicates that the increased filling pressure of the right heart results in increased cardiac output.
The LaPlace law states that wall stress is proportional to pressure and chamber size and inversely proportional to wall thickness. The Young-Laplace equation can be used to calculate afterload by determining the wall stress of the left ventricle. According to LaPlace's law, the tension upon the muscle fibres in the heart wall is the pressure within the ventricle multiplied by the volume within the ventricle, divided by the wall thickness.
In the context of mitral regurgitation, the LaPlace formula is important in understanding the various states of MR that can alter oxygen demand, resulting in subendocardial ischaemia and, subsequently, dyspnoea. Left ventricular (LV) wall stress-volume loops can be observed in the three stages of chronic mitral regurgitation. Increased LV end-diastolic volume and pressure will result in an increased LV end-diastolic wall stress. This increased wall stress may cause subendocardial ischaemia and subsequently myocardial fibrosis.
Law Office Notarization: Validating Your Will
You may want to see also
Frequently asked questions
Mitral regurgitation (MR) is the most common valvular heart disease. It is a complex multifactorial disease that involves multiple entities.
In patients with hypertrophic cardiomyopathy, mitral regurgitation is caused by mitral systolic anterior motion (SAM). SAM produces greater mitral regurgitation if the posterior leaflet is limited in its ability to move anteriorly.
Until the 1980s, mitral regurgitation was diagnosed by right heart catheterisation in combination with left ventricular cine-angiography. The advancement of echocardiographic techniques, such as Doppler measurements, eventually replaced invasive and angiographic methods.
The Law of Laplace describes the factors that determine left ventricular wall stress, which is a major determinant of myocardial oxygen demand. Increased wall tension in the ventricles can lead to cardiac hypertrophy and may compromise coronary blood flow. The Law of Laplace is important in understanding the various states of MR that can alter oxygen demand, resulting in subendocardial ischaemia and dyspnoea.