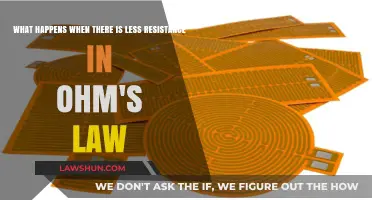
When a person loses a lung, the body’s ability to exchange gases—oxygen and carbon dioxide—is significantly compromised, and this can be understood through the lens of Fick's Law of Diffusion. Fick's Law states that the rate of gas exchange across a membrane is directly proportional to the surface area available for diffusion, the concentration gradient of the gas, and the diffusion coefficient, while inversely proportional to the thickness of the membrane. With the loss of a lung, the total surface area for gas exchange is halved, reducing the body’s capacity to absorb oxygen and eliminate carbon dioxide. This decrease in surface area directly impacts the rate of diffusion, leading to hypoxia (low oxygen levels) and potential hypercapnia (high carbon dioxide levels). The remaining lung may compensate to some extent by increasing blood flow and enhancing ventilation, but the overall efficiency of gas exchange is still diminished, often necessitating medical interventions to support respiratory function.
| Characteristics | Values |
|---|---|
| Oxygen Diffusion Capacity | Reduced by approximately 50% due to decreased surface area for gas exchange. |
| Pulmonary Blood Flow | Redistributed to the remaining lung, increasing its workload. |
| Ventilation-Perfusion (V/Q) Mismatch | Increased mismatch due to loss of lung tissue, leading to hypoxemia. |
| Fick's Law Application | Oxygen uptake (VO2) is compromised as diffusion distance and area decrease. |
| Respiratory Rate | May increase to compensate for reduced oxygen uptake. |
| Heart Rate and Blood Pressure | Potential increase due to compensatory mechanisms to maintain oxygen delivery. |
| Exercise Tolerance | Significantly reduced due to decreased oxygen availability. |
| Carbon Dioxide Elimination | May be impaired if the remaining lung cannot compensate fully. |
| Long-Term Adaptation | Remaining lung may hypertrophy over time to improve function. |
| Survival and Quality of Life | Varies; depends on overall health, remaining lung function, and adaptations. |
Explore related products






What You'll Learn
- Gas Exchange Reduction: Fick's Law shows decreased diffusion capacity due to reduced surface area post-lung loss
- Oxygen Uptake Limitation: Lower partial pressure gradient impacts oxygen uptake efficiency in remaining lung tissue
- Carbon Dioxide Retention: Impaired CO2 elimination due to reduced ventilation-perfusion matching in single-lung scenarios
- Cardiovascular Strain: Increased pulmonary pressure and right heart workload from altered blood flow dynamics
- Compensatory Mechanisms: Remaining lung hyperinflation and increased respiratory rate to offset diffusion limitations
![]()
Gas Exchange Reduction: Fick's Law shows decreased diffusion capacity due to reduced surface area post-lung loss
When an individual loses a lung, the body experiences a significant reduction in the surface area available for gas exchange, which directly impacts respiratory function. Fick's Law of Diffusion, a fundamental principle in physiology, explains how the rate of gas exchange across a membrane is proportional to the surface area available for diffusion, the concentration gradient of the gas, and the diffusion coefficient of the gas. With the loss of a lung, the surface area for gas exchange is halved, leading to a substantial decrease in the body's ability to efficiently exchange oxygen and carbon dioxide. This reduction in surface area becomes the primary driver of diminished diffusion capacity, as there is less alveolar-capillary interface through which gases can move.
The decreased surface area post-lung loss directly translates to a reduced diffusion capacity, as Fick's Law highlights the critical role of surface area in gas exchange. Normally, the vast surface area of the alveoli in both lungs ensures that oxygen can diffuse into the bloodstream and carbon dioxide can exit efficiently. However, with only one lung, the remaining alveoli must compensate for the lost capacity, which they cannot fully achieve due to the physical limitation of reduced surface area. This inefficiency results in lower oxygen saturation in the blood and higher carbon dioxide levels, as the rate of gas exchange is insufficient to meet the body's metabolic demands.
Fick's Law also emphasizes the importance of the concentration gradient in gas exchange. While the concentration gradient itself may remain relatively unchanged post-lung loss, the reduced surface area limits the overall amount of gas that can diffuse per unit of time. This means that even if the partial pressure differences between alveolar air and blood remain optimal, the total volume of gas exchanged is significantly lower. Consequently, the body must work harder to maintain adequate oxygenation, often leading to increased respiratory rates and depths as the remaining lung attempts to compensate for the loss.
The practical implications of reduced diffusion capacity due to decreased surface area are profound. Patients with a single lung often experience dyspnea (shortness of breath), fatigue, and reduced exercise tolerance, as the body struggles to meet its oxygen requirements during physical activity. Additionally, the increased workload on the remaining lung can lead to long-term complications, such as pulmonary hypertension and right-sided heart failure, as the cardiovascular system adapts to the chronic hypoxia. These outcomes underscore the critical relationship between surface area and gas exchange efficiency, as described by Fick's Law.
In summary, the loss of a lung results in a significant reduction in gas exchange capacity, primarily due to the halved surface area available for diffusion. Fick's Law provides a clear framework for understanding this phenomenon, highlighting how the decreased alveolar-capillary interface limits the rate of oxygen and carbon dioxide exchange. This reduction in diffusion capacity manifests clinically as respiratory symptoms and systemic complications, emphasizing the indispensable role of surface area in maintaining adequate pulmonary function. Understanding these principles is crucial for managing patients with a single lung and optimizing their respiratory care.
The Decline of Man Laws: A Cultural Shift Explored
You may want to see also
Explore related products






![]()
Oxygen Uptake Limitation: Lower partial pressure gradient impacts oxygen uptake efficiency in remaining lung tissue
When an individual loses a lung, the remaining lung tissue must compensate for the reduced respiratory capacity. This scenario directly relates to Fick's Law of Diffusion, which states that the rate of gas exchange across a membrane is proportional to the partial pressure gradient of the gas, the surface area available for diffusion, and the diffusion capacity of the membrane. In the context of oxygen uptake, the partial pressure gradient of oxygen (PO₂) between alveolar air and pulmonary capillary blood is a critical determinant of diffusion efficiency. With the loss of a lung, the total surface area for gas exchange is significantly reduced, but equally important is the alteration in the partial pressure gradient that drives oxygen diffusion.
The partial pressure of oxygen in the alveoli (PAO₂) is typically higher than that in the blood, creating a gradient that facilitates oxygen movement into the bloodstream. However, when lung tissue is lost, the remaining lung must work harder to maintain adequate oxygenation. The lower total surface area means that the remaining alveoli are exposed to a higher volume of blood flow per unit area, which can reduce the time available for oxygen diffusion. Additionally, the partial pressure gradient may decrease because the remaining lung tissue is less efficient at ventilating and perfusing blood, leading to a mismatch between ventilation and perfusion (V/Q mismatch). This mismatch further diminishes the effective PO₂ gradient, impairing oxygen uptake efficiency.
Fick's Law highlights that a reduced partial pressure gradient directly limits the rate of oxygen diffusion. In a healthy lung, the steep gradient between alveolar oxygen and deoxygenated blood ensures rapid oxygen uptake. However, with the loss of a lung, the remaining tissue may struggle to maintain this gradient due to increased physiological demands and reduced alveolar-capillary interface efficiency. The body attempts to compensate by increasing cardiac output or respiratory rate, but these mechanisms cannot fully restore the lost diffusion capacity. As a result, the remaining lung tissue operates at a suboptimal PO₂ gradient, leading to decreased oxygen uptake efficiency and potential hypoxemia.
Another critical factor is the redistribution of blood flow to the remaining lung. While this redistribution aims to maximize oxygenation, it can exacerbate regional differences in ventilation and perfusion. Areas of the lung that are overperfused relative to ventilation experience a lower local PO₂ gradient, further reducing oxygen diffusion. This regional inefficiency contributes to the overall limitation in oxygen uptake, as the remaining lung tissue cannot uniformly maintain the necessary partial pressure gradient across all alveoli. Thus, the loss of a lung not only reduces surface area but also disrupts the delicate balance required for efficient gas exchange.
In summary, the limitation in oxygen uptake following the loss of a lung is significantly influenced by the lower partial pressure gradient of oxygen in the remaining lung tissue. Fick's Law underscores that a diminished gradient directly impairs diffusion efficiency, even as the body attempts to compensate through increased blood flow or respiratory effort. The resulting V/Q mismatch and regional inefficiencies further reduce the effective PO₂ gradient, compounding the challenge of maintaining adequate oxygenation. Understanding these principles is essential for managing respiratory function in individuals with reduced lung capacity and highlights the critical role of the partial pressure gradient in gas exchange dynamics.
Indian Succession Law: CK2 Explained
You may want to see also
Explore related products






![]()
Carbon Dioxide Retention: Impaired CO2 elimination due to reduced ventilation-perfusion matching in single-lung scenarios
When an individual loses a lung, the remaining lung must compensate for the reduced respiratory capacity, leading to significant changes in gas exchange dynamics. Carbon dioxide (CO₂) retention becomes a critical concern due to impaired CO₂ elimination, primarily caused by reduced ventilation-perfusion (V/Q) matching. Fick's Law of diffusion, which states that gas exchange is directly proportional to the partial pressure gradient and the surface area available for diffusion, highlights the importance of balanced ventilation and perfusion for efficient CO₂ removal. In a single-lung scenario, the remaining lung faces increased demands, often resulting in mismatched ventilation and perfusion, where blood flow (perfusion) exceeds air delivery (ventilation) in certain regions.
In normal physiology, V/Q matching ensures that oxygen and CO₂ are exchanged optimally in the alveoli. However, with the loss of one lung, the remaining lung's capacity to ventilate and perfuse evenly is compromised. This mismatch leads to shunt-like effects, where deoxygenated blood bypasses ventilated areas, reducing the efficiency of CO₂ elimination. The partial pressure gradient for CO₂, which drives its diffusion from blood to alveoli, is disrupted, as the remaining lung struggles to maintain adequate alveolar ventilation. Consequently, CO₂ accumulates in the bloodstream, leading to hypercapnia, a condition characterized by elevated arterial CO₂ levels.
The impaired CO₂ elimination in single-lung scenarios is further exacerbated by the increased physiological workload on the remaining lung. The lung must expand its capacity to meet the body's oxygen demands while simultaneously clearing CO₂. However, the reduced surface area for gas exchange limits its ability to maintain the necessary diffusion gradient. Fick's Law underscores that diffusion is directly proportional to the surface area, and with half the alveolar surface area lost, the remaining lung cannot compensate fully, leading to retention of CO₂.
Clinically, this retention manifests as respiratory acidosis, as the body attempts to buffer excess CO₂ by retaining bicarbonate ions, disrupting acid-base balance. Patients may experience symptoms such as dyspnea, confusion, and fatigue due to hypercapnia. Management strategies focus on optimizing V/Q matching through mechanical ventilation techniques, such as positive end-expiratory pressure (PEEP), to improve alveolar recruitment and reduce shunting. Additionally, supplemental oxygen is often administered to enhance the partial pressure gradient for CO₂ elimination, though it does not directly address the underlying V/Q mismatch.
In summary, carbon dioxide retention in single-lung scenarios is a direct consequence of impaired CO₂ elimination due to reduced ventilation-perfusion matching. Fick's Law emphasizes the critical role of surface area and partial pressure gradients in gas exchange, both of which are compromised when one lung is lost. Understanding these principles is essential for developing effective interventions to mitigate hypercapnia and its associated complications in patients with reduced lung capacity.
No Basis in Law: Consequences of a Judge's Determination
You may want to see also
Explore related products






![]()
Cardiovascular Strain: Increased pulmonary pressure and right heart workload from altered blood flow dynamics
When an individual loses a lung, the cardiovascular system undergoes significant strain due to altered blood flow dynamics, which can be understood through Fick's Law of Diffusion. Fick's Law describes the relationship between gas exchange, blood flow, and the partial pressure gradient of gases. Normally, the lungs facilitate oxygen and carbon dioxide exchange based on the principle that gases move from areas of higher partial pressure to areas of lower partial pressure. With the loss of a lung, the remaining lung must compensate for the reduced surface area and alveolar volume, leading to increased pulmonary vascular resistance and altered blood flow dynamics. This compensation mechanism places a substantial burden on the cardiovascular system, particularly the right side of the heart.
The immediate consequence of losing a lung is a reduction in the total cross-sectional area available for gas exchange. According to Fick's Law, the rate of gas exchange is directly proportional to the surface area and the partial pressure gradient. With a smaller lung volume, the remaining lung must increase blood flow to maintain adequate oxygenation. However, this increased blood flow is constrained by the reduced alveolar surface area, leading to higher pulmonary vascular resistance. As resistance increases, the right ventricle must work harder to pump blood through the pulmonary circulation, resulting in elevated pulmonary artery pressures. This increased workload on the right heart can lead to right ventricular hypertrophy and, over time, right heart failure if the strain is not alleviated.
The altered blood flow dynamics also disrupt the normal distribution of blood within the pulmonary vasculature. In a healthy individual, blood flow is matched to areas of the lung with the highest ventilation, ensuring efficient gas exchange. However, with the loss of a lung, blood flow becomes unevenly distributed, as the remaining lung must accommodate the entire cardiac output. This mismatch between ventilation and perfusion (V/Q mismatch) further exacerbates hypoxia and increases the workload on the right heart. The body attempts to compensate by vasoconstricting pulmonary arteries in under-ventilated areas, but this mechanism contributes to the overall increase in pulmonary vascular resistance and pressure.
Chronic cardiovascular strain from increased pulmonary pressure can lead to cor pulmonale, a condition characterized by right ventricular enlargement and dysfunction. The right ventricle, which is not as muscular or robust as the left ventricle, is particularly vulnerable to sustained pressure overload. As the right heart struggles to pump blood against elevated pulmonary pressures, systemic venous congestion may occur, leading to symptoms such as peripheral edema, ascites, and hepatomegaly. Additionally, the increased afterload on the right ventricle can impair its ability to fill adequately, further reducing cardiac output and exacerbating hypoxia.
Managing cardiovascular strain in individuals with a single lung requires a multifaceted approach. Therapies aimed at reducing pulmonary vascular resistance, such as oxygen supplementation and pulmonary vasodilators, can help alleviate the workload on the right heart. In severe cases, mechanical ventilation or extracorporeal membrane oxygenation (ECMO) may be necessary to support gas exchange and reduce the strain on the cardiovascular system. Long-term management often involves monitoring for signs of right heart failure and implementing lifestyle modifications to optimize cardiac function. Understanding the principles of Fick's Law and the resulting blood flow dynamics is crucial for developing effective strategies to mitigate the cardiovascular consequences of lung loss.
Is Wearing a Bike Helmet Required by California Law?
You may want to see also
Explore related products






![]()
Compensatory Mechanisms: Remaining lung hyperinflation and increased respiratory rate to offset diffusion limitations
When an individual loses a lung, the remaining lung must compensate for the significant reduction in respiratory surface area, which directly impacts gas exchange. According to Fick's Law of Diffusion, the rate of gas exchange is proportional to the surface area available for diffusion, the concentration gradient of the gas, and the diffusion capacity of the membrane. With the loss of one lung, the surface area for gas exchange is halved, creating a critical limitation in oxygen and carbon dioxide exchange. To offset this, the body employs compensatory mechanisms, primarily involving hyperinflation of the remaining lung and an increased respiratory rate.
Hyperinflation of the remaining lung is a key compensatory mechanism. The lung stretches beyond its normal volume to maximize the surface area available for gas exchange. This is achieved through increased inspiratory effort, allowing more alveoli to participate in diffusion. Hyperinflation helps maintain a larger concentration gradient for oxygen and carbon dioxide, partially mitigating the reduced surface area. However, this mechanism is not without limitations, as excessive stretching can lead to alveolar damage and decreased compliance, reducing the lung's efficiency over time.
An increased respiratory rate is another critical compensatory response. By breathing more frequently, the individual can enhance the overall volume of air moving in and out of the lungs per minute, known as the minute ventilation. This compensates for the reduced surface area by ensuring that a greater volume of air is exposed to the remaining alveolar surface, thereby increasing the opportunity for gas exchange. However, this mechanism also has drawbacks, as rapid breathing can lead to respiratory muscle fatigue and inefficient gas exchange due to reduced time for diffusion during each breath.
These compensatory mechanisms are governed by the principles of Fick's Law, as they aim to optimize the remaining functional parameters—surface area, concentration gradient, and time—to maintain adequate gas exchange. While hyperinflation and increased respiratory rate can partially offset the diffusion limitations caused by the loss of a lung, they are not perfect solutions. The body must work harder to achieve the same level of gas exchange, often leading to increased metabolic demand and potential long-term strain on the respiratory system.
In summary, the compensatory mechanisms of remaining lung hyperinflation and an increased respiratory rate are essential for maintaining gas exchange after the loss of a lung. These mechanisms directly address the diffusion limitations imposed by reduced surface area, as described by Fick's Law. However, they are not without limitations and highlight the remarkable adaptability of the human respiratory system in the face of significant physiological challenges. Understanding these mechanisms is crucial for managing patients with reduced lung capacity and optimizing their respiratory function.
The Ethical Dilemma: Should Anti-Semitic Laws Exist in Society?
You may want to see also
Frequently asked questions
Fick's Law describes the rate of gas exchange across a membrane, such as the alveolar-capillary interface in the lungs. It states that gas exchange is proportional to the surface area, the concentration gradient, and the diffusion coefficient, and inversely proportional to the membrane thickness. When you lose a lung, the reduced surface area directly impacts gas exchange efficiency.
Losing a lung reduces the total surface area available for gas exchange. According to Fick's Law, a decrease in surface area lowers the rate of oxygen diffusion into the bloodstream, potentially leading to hypoxemia (low blood oxygen levels).
The remaining lung can partially compensate by increasing its surface area through hyperinflation and enhancing blood flow to functional alveoli. However, this compensation is limited, as Fick's Law dictates that gas exchange is directly proportional to surface area, which remains reduced after lung loss.
Similar to oxygen uptake, carbon dioxide elimination is impaired due to reduced surface area. Fick's Law indicates that the rate of CO2 diffusion from the blood to the alveoli decreases, potentially leading to hypercapnia (elevated blood CO2 levels).
Yes, Fick's Law helps explain shortness of breath in patients with one lung. The reduced surface area for gas exchange limits oxygen uptake and CO2 elimination, forcing the body to work harder to meet metabolic demands, resulting in increased respiratory effort and breathlessness.